When someone collapses in cardiac arrest, the fastest path to a better outcome is not rhythm debate. It is a decisive action: start CPR, attach an AED, and follow prompts with minimal interruptions. Rhythm terms like asystole and V-fib matter because they explain why an AED may advise a shock in one situation and not in another.
In workplaces, schools, gyms, and public facilities, responders are not expected to interpret ECG strips. AEDs are designed to do the rhythm analysis and guide the response. The most important thing an organization can do is build a rescue-ready program—clear access, trained responders, and equipment that stays in a verified ready status year-round.
For context, the American Heart Association’s adult cardiac arrest algorithm separates shockable rhythms (VF/pVT) from non-shockable rhythms (asystole/PEA) and reinforces high-quality CPR with minimal pauses between rhythm checks. That “keep compressions going” priority is the heart of AED response in real environments.
Asystole Vs V-Fib At A Glance
The simplest way to understand these rhythms is to compare what they represent and what the AED response typically looks like. This isn’t meant to turn bystanders into clinicians. It’s meant to make AED prompts feel logical so teams stay calm and consistent during a real emergency.
| Feature | Ventricular Fibrillation (V-Fib) | Asystole |
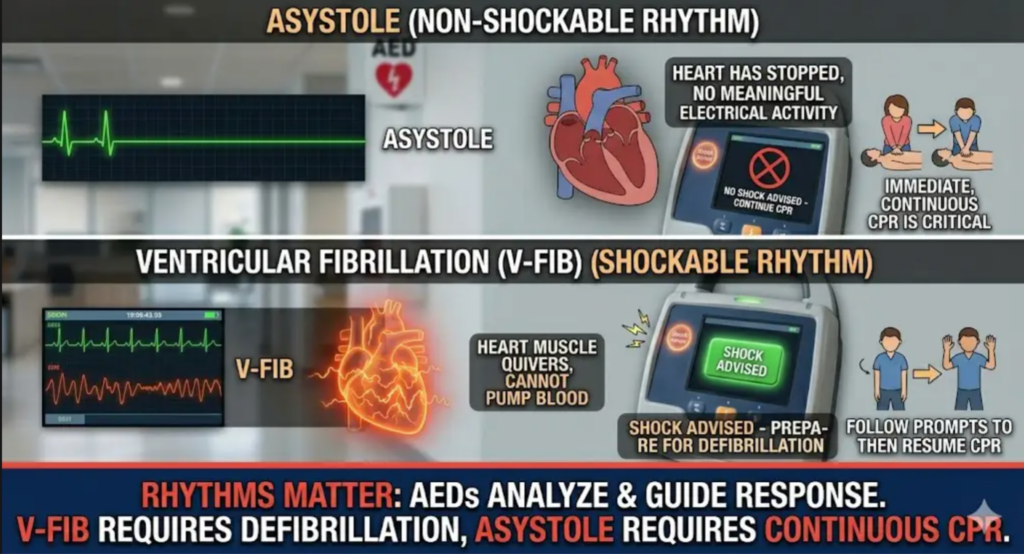
| What’s happening | Chaotic electrical activity; ventricles quiver instead of pumping | No meaningful ventricular electrical activity (“flatline”) |
| Shockable rhythm? | Usually Yes | No |
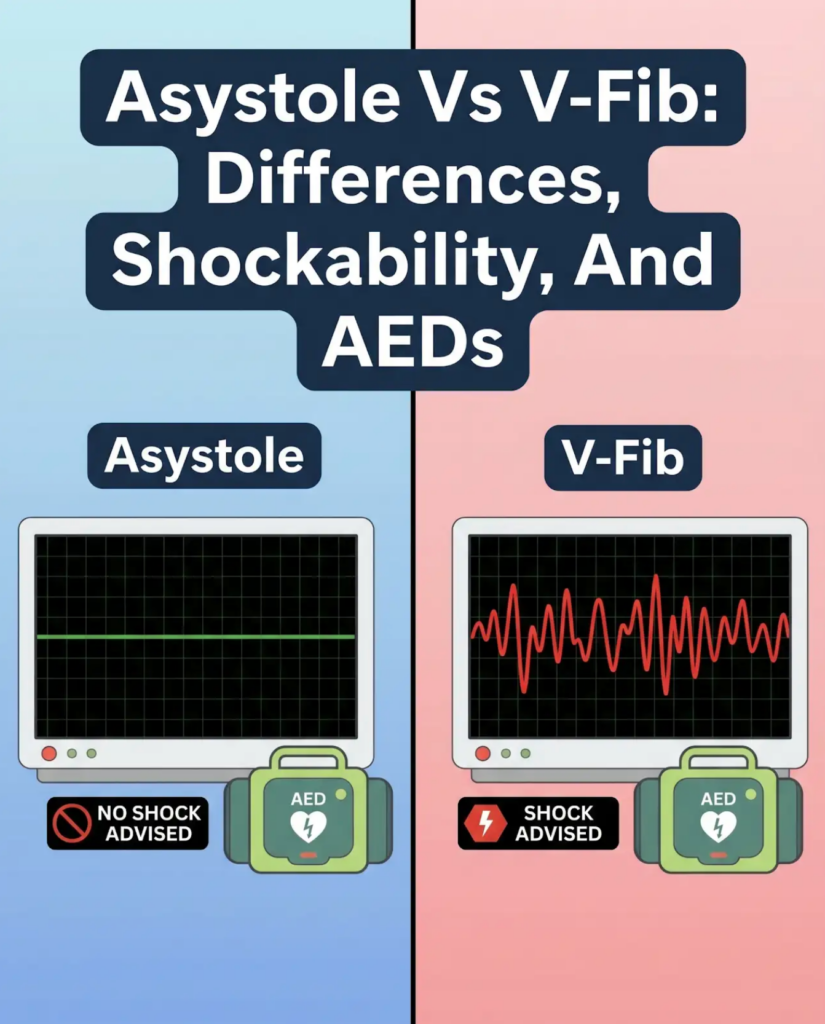
| What an AED may say | “Shock advised” (if VF pattern detected) | “No shock advised” (CPR continues) |
| Most important bystander action | CPR + AED early; shock if advised; resume CPR immediately | CPR immediately; follow AED prompts; minimize interruptions |
| Why it matters | Defibrillation can interrupt chaos and allow organized rhythm to return | Defibrillation isn’t indicated; CPR and advanced care are critical |
| Common confusion | Fine VF can look small and “flat” on poor signal | Artifact/lead issues can mimic flatline in clinical settings |
V-fib is chaotic electrical activity in the ventricles. Because there is disorganized electrical activity that may respond to defibrillation, it is treated as a shockable rhythm in standard resuscitation pathways. Asystole is the absence of meaningful ventricular electrical activity, and it is not shockable—the response centers on high-quality CPR and rapid escalation to advanced care.
If your AED says “shock advised,” follow the shock prompts and return to CPR immediately. If your AED says “no shock advised,” resume CPR immediately and follow re-analysis prompts. The AHA algorithm emphasizes short rhythm checks and immediate compressions regardless of the pathway.
What This Means For AED Responders
AED users do not need to diagnose rhythms. The device analyzes rhythm and advises shocks only when indicated, which is why AED training is built around a repeatable sequence rather than interpretation. The Red Cross outlines that practical sequence—check, call, turn on AED, apply pads, and follow prompts—which matches how most workplace responders are taught to operate under pressure (Red Cross AED Steps).
What These Rhythms Mean In Plain Terms
It helps to think of cardiac arrest response as two priorities running at the same time. CPR provides circulation support, and the AED determines whether defibrillation can help restore an organized rhythm. Both asystole and V-fib are cardiac arrest emergencies. The difference is whether a shock is part of the treatment pathway.
When teams understand that difference, they trust the AED and stay focused on compressions and timing. That’s how the system is designed to work.
What Is Ventricular Fibrillation (V-Fib)?
V-fib occurs when the ventricles have chaotic electrical signals, causing them to quiver rather than pump blood. This can lead to collapse and loss of circulation, which is why it is treated as a life-threatening rhythm that often requires immediate defibrillation plus CPR. Often V-fib as an abnormal rhythm that prevents the lower chambers from pumping blood effectively and requires immediate medical care.
What Is Asystole?
Asystole is commonly described as “flatline,” reflecting a lack of meaningful ventricular electrical activity. In this situation, defibrillation is not indicated, and the response focuses on uninterrupted CPR and advanced interventions by trained professionals. Asystole is described as the failure of the heart’s electrical system that results in the heart stopping and a flatline pattern on an ECG.
Shockable Vs Non-Shockable Rhythms
“Shockable” does not mean “more survivable,” and “non-shockable” does not mean “nothing can be done.” These labels simply describe whether defibrillation is part of the recommended pathway based on the rhythm pattern.
For workplace response, the value of this distinction is practical: it helps responders understand why the AED is giving specific instructions. That understanding reduces hesitation and keeps the team moving.
Why AEDs Don’t Shock Asystole
Defibrillation is designed to interrupt certain chaotic rhythms so an organized rhythm can return. In asystole, there is no shockable rhythm to reset. That’s why AEDs will not advise shocks for asystole and will guide responders back to CPR with timed re-analysis. The “no shock advised → resume CPR” cycle is reflected in the AHA algorithm’s non-shockable pathway.
What “Shock Advised” And “No Shock Advised” Really Mean
When the AED says “shock advised,” it has detected a rhythm pattern consistent with shockable VF or pulseless VT and is guiding shock delivery, then immediate CPR. When it says “no shock advised,” it has not detected a shockable rhythm at that moment, and the priority remains compressions and re-analysis on the device’s cadence. This is why most algorithms treat pauses as brief and keep CPR at the center of the response.
Fine V-Fib Vs Asystole
Fine VF is where a lot of confusion starts. People hear “flatline” and assume “shock won’t help,” but very low-amplitude VF can look close to a flatline on quick assessment. This nuance is mostly relevant for clinicians using manual monitors, but it also reinforces a core rule for workplace response: don’t guess—follow the AED.
Advanced life support guidance highlights that rhythm checks should be brief and CPR interruptions minimized, even when VF is fine or difficult to distinguish. That “compressions first” principle protects the patient while the device or clinical team confirms the pathway.
Why Fine V-Fib Causes Confusion
Fine VF means the chaotic electrical activity is present, but the wave amplitude is small. On a single lead, poor signal, or artifact, it can be harder to distinguish from asystole. Clinician-focused rhythm education often emphasizes confirming signal quality and minimizing unnecessary pauses in compressions when there is doubt.
What Workplace Teams Should Do Instead Of Guessing
In the workplace response, the best use of time is compressions and AED application—not rhythm interpretation. Start CPR, attach pads, and follow prompts. If “no shock advised,” keep compressions going and allow the AED to re-analyze. If “shock advised,” follow the shock sequence and return to CPR immediately.
This is exactly why training should match what responders will see in your building. Life Support Systems provides on-site and flexible instruction through Training so teams practice the same AED response flow they’ll use during a real emergency.
How V-Fib Can Progress Into Asystole
One reason early defibrillation is emphasized in shockable rhythms is that untreated VF can deteriorate. Over time, VF can become finer and may transition into non-shockable rhythms, including asystole. The practical implication for workplaces is urgency: rapid CPR and early AED application improve the chance that a shockable rhythm is identified and treated early.
Resuscitation pathways reinforce that urgency by alternating short rhythm checks with two-minute CPR cycles, pushing responders back into compressions quickly after either a shock or a no-shock decision.
What To Do In The Workplace
Workplace response succeeds when speed is paired with structure. A team that knows the first steps and follows them without hesitation can make a meaningful difference before EMS arrives. The rhythms matter, but the response fundamentals matter more.
If your facility has an AED program, the goal is not only to have a device on-site. The goal is to ensure the AED is visible, accessible, and ready, and that responders have the confidence to act.
Immediate Response Steps That Apply In Both Rhythms
In both V-fib and asystole, your initial actions are the same: activate emergency response, start CPR, get the AED to the patient, apply pads, and follow prompts. The AED will decide shock vs no shock. Your job is to keep compressions going whenever instructed, because circulation support is essential while rhythm checks happen.
That same sequence is reinforced across major responder training frameworks, including the simplified public steps described by the Red Cross (Red Cross AED Steps).
After Any Use: Return The AED To Ready Status
After a response, the AED must be reset and verified as ready. Pads should be replaced, battery status should be checked, the cabinet should be restored and accessible, and the readiness indicator should be confirmed before the unit is considered back in service.
This “return-to-ready” process is where many programs quietly fail, especially when replacements aren’t tracked or there’s no clear owner. For ongoing inspections, replacement planning, and readiness verification, Life Support Systems supports programs through AED Maintenance & Service.
Common Myths And Mistakes
Most AED failures aren’t device failures. They’re program breakdowns that create delays, confusion, or a non-ready unit when it matters most. Clearing up a few myths can materially improve real-world performance.
The most reliable programs remove uncertainty through training, placement, and routine checks, so the response remains simple even under stress.
“Shock The Flatline”
A persistent misconception is that a flatline should be shocked. Asystole is not treated with defibrillation in standard pathways, and AEDs are designed not to advise shocks in that scenario. The correct action is CPR, rapid escalation to advanced care, and following AED prompts for re-analysis. It has been shown that asystole represents a failure of the heart’s electrical system and is a cardiac arrest condition requiring immediate intervention, just not defibrillation as the primary tool.
Long Pauses In CPR
Extended pauses for analysis, discussion, or repeated checks reduce the quality of the response. AED prompts are built to minimize that risk, but only if teams follow the “resume CPR” instruction immediately. The AHA pathway repeatedly drives responders back into compressions after each decision point.
Readiness Gaps That Trigger “Not Ready” At The Worst Time
Expired pads, depleted batteries, blocked cabinets, and missing accessories are the silent failures that derail real rescues. The solution isn’t complicated. It’s consistent tracking, monthly readiness checks, and clear ownership—exactly what a maintenance program is designed to support.
How Life Support Systems Helps
A workplace doesn’t need to be able to diagnose rhythms to run a strong AED program. It needs fast access, trained responders, and equipment that stays rescue-ready. Life Support Systems supports AED readiness through equipment guidance, training, on-site service, and replacement planning, with programs built for one site or nationwide operations.
If you want a practical review of your current AED readiness—placement, training coverage, and maintenance cadence—the fastest next step is to contact us. We’ll help you identify gaps and build a clear plan that keeps AED response simple when seconds matter.
FAQs
Is Asystole Shockable?
No. Asystole is not shockable in standard adult cardiac arrest pathways, and AEDs will advise “no shock” while directing continued CPR.
Is Ventricular Fibrillation Shockable?
Yes. V-fib is typically treated as shockable, and early defibrillation is a core part of shockable-rhythm response.
Can An AED Shock Asystole?
No. AEDs are designed to advise shocks only when a shockable rhythm is detected and to direct CPR when a shock is not indicated..
What Does “Shock Advised” Mean?
It means the AED detected a shockable rhythm pattern and is guiding shock delivery followed by immediate CPR cycles.
What Does “No Shock Advised” Mean?
It means a shock is not indicated at that moment. CPR should resume immediately, and the AED will re-analyze on its cadence.
What Is Fine V-Fib?
Fine V-fib is low-amplitude VF that can be harder to distinguish on poor signal in clinical settings, which is why advanced guidance emphasizes minimizing CPR interruptions and following the shockable/non-shockable pathway carefully.
What Should We Do If The AED Says “No Shock Advised”?
Resume CPR immediately and follow the AED prompts. Do not stop repeatedly to recheck unless the device instructs you to do so (Red Cross AED Steps).
How Can A Workplace Keep AEDs Rescue-Ready?
Visible placement, role-based training, monthly readiness checks, and tracking pad/battery replacement dates keep AEDs ready. Ongoing support is available through Training and AED Maintenance & Service.
Last updated on 3 days ago